Patient discussion aid
Points to cover during discussion with patient about antibiotic prophylaxis
It is important that patients are not discouraged from undergoing dental treatment.
For patients at high risk and moderate risk of infective endocarditis (see Patients at risk of infective endocarditis):
Advise the patient that due to their heart condition/previous episode of infective endocarditis, they have an increased risk of developing infective endocarditis following an ‘at-risk’ dental procedure.
- Explain that infective endocarditis is a very rare but serious infection of the lining of the heart, often involving the heart valves, caused mainly by bacteria which enter the bloodstream from outside the body (bacteraemia).
- Explain that if the patient develops infective endocarditis, they are also at increased risk of developing complications and have an increased risk of morbidity and mortality.
Explain that having an ‘at-risk’ dental procedure, such as an extraction, may increase the chances of bacteria entering the bloodstream.
- The tables below provide estimates of the risk of developing infective endocarditis after an ‘at-risk’ dental procedure in the absence of antibiotic prophylaxis for different patient groups and for specific ‘at-risk’ dental procedures (i.e. extractions and oral surgery) in high risk patients.
Estimated risk of developing infective endocarditis after an ‘at-risk’ dental procedure in specific patient groups in the absence of antibiotic prophylaxis31
| Patient Group | Low/unknown risk | Moderate risk | High risk |
|---|---|---|---|
| Estimated risk of IE | 1 in 333,000 | 1 in 50,000 | 1 in 1,000 |
Estimated risk of developing infective endocarditis after extractions and oral surgery procedures in high risk patients in the absence of antibiotic prophylaxis31
| Dental procedure | Extraction | Oral surgery |
|---|---|---|
| Estimated risk of IE | 1 in 100 | 1 in 40 |
The figure below may help you to explain risk to patients.
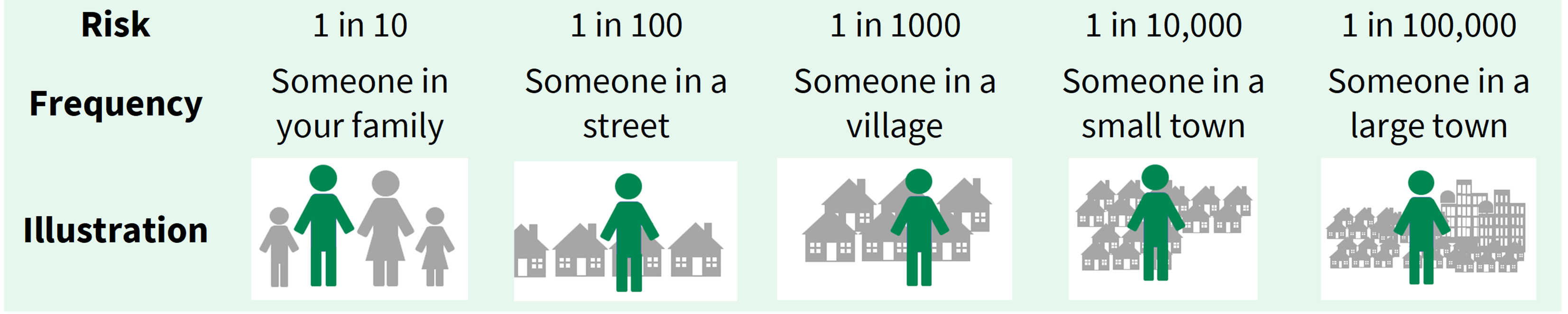
Adapted from Risk Language and Dialects, Calman and Royston, BMJ 1997; 315:939
Explain that everyday activities, such as toothbrushing, flossing and chewing can also cause transient bacteraemias and stress the importance of good oral hygiene to reduce the risk of this.
Give advice on prevention of infective endocarditis to all high and moderate risk patients.
- Explain the importance of maintaining good oral health to prevent infective endocarditis.
- Emphasise that good oral hygiene is the best way to prevent oral diseases that could require treatment with ‘at-risk’ dental procedures and will also reduce the chance of oral bacteria getting into the blood stream during everyday activities.
- Provide personalised oral hygiene advice and instruction to assist and encourage the patient to improve their oral hygiene skills.
- Advise the patient to reduce the frequency of sugary snacks/drinks to prevent tooth decay.
- Highlight the importance of regular dental check-ups to ensure that any dental disease is treated before ‘at-risk’ dental procedures are required.
- Explain that undergoing invasive procedures, including non-medical procedures such as body piercing or tattooing may also increase their risk of infective endocarditis.
The potential benefits and harms of antibiotic prophylaxis against infective endocarditis should be discussed with the patient to facilitate shared decision making.
For high risk patients, explain that antibiotic prophylaxis before ‘at-risk’ dental procedures is recommended or should be considered for them, depending on the dental procedure.
- There is evidence that some dental procedures (i.e. extractions and oral surgery procedures) may significantly increase their risk of infective endocarditis and antibiotic prophylaxis should be offered for these procedures.
- It is unclear whether dental procedures that that involve manipulation of the gingival (i.e. gums) or periapical region of a tooth (i.e. root tip) will increase their risk of infective endocarditis and antibiotic prophylaxis should be considered for these procedures. This must involve reaching a shared decision with the patient and consideration of their oral health status.
- Antibiotic prophylaxis does not fully eliminate the risk of infective endocarditis.
- Antibiotics can cause side effects, such as nausea, diarrhoea and allergic reactions and, in rare cases, anaphylaxis and antibiotic-related colitis which can be fatal.
- It may also be helpful to discuss the issues surrounding antibiotic resistance (see Prescribing advice).
For moderate risk patients, explain that antibiotic prophylaxis before ‘at-risk’ dental procedures is not recommended for them.
- There is no evidence that antibiotic prophylaxis will reduce their risk of infective endocarditis.
- Antibiotic prophylaxis does not fully eliminate the risk of infective endocarditis.
- Antibiotics can cause side effects, such as nausea, diarrhoea and allergic reactions and, in rare cases, anaphylaxis and antibiotic-related colitis which can be fatal.
- It may also be helpful to discuss the issues surrounding antibiotic resistance (see Prescribing advice).
Advise all high and moderate risk patients to contact their general medical practitioner as soon as possible if they notice any of the following symptoms of infective endocarditis, particularly if they occur together as a flu-like illness:
-
- a high temperature (fever) of 38oC or above
- sweats or chills, especially at night
- breathlessness, especially during physical activity
- weight loss
- tiredness (fatigue)
- muscle, joint or back pain (unrelated to recent physical activity)
- Emphasise that these symptoms are more likely to be caused by a less serious type of infection but should be investigated.
- Ensure that the patient knows to tell any medical professional they seek advice from about any recent dental treatment they may have had.
Ensure that patients prescribed antibiotic prophylaxis are aware of the potential for hypersensitivity, anaphylaxis or antibiotic-associated colitis and that they should seek urgent medical attention if they later develop colitis (diarrhoea), which can be fatal.
Record all discussions with the patient in their clinical notes.